Synthetic cannabis
Prevalence of use among offenders, perception of risk and negative side effects experienced
Sarah Macgregor and Jason Payne
Key Points
- Of 871 police detainees surveyed through the Drug Use Monitoring in Australia (DUMA) program, 4 per cent reported recent use of synthetic cannabis. This compares to almost half (46%) who reported recent use of natural cannabis
- The most common source for obtaining synthetic cannabis (aside from ‘a friend’) was from some type of shop (42%) such as a tobacconist or sex shop
- At the time of interview, several synthetic compounds had been added to Schedule nine of the 2011 Commonwealth Poisons Standard by the TGA and statewide bans on the possession and distribution of synthetic cannabis products had occurred in every jurisdiction. However over half (60%) of users still believed synthetic cannabis was legal to buy at the time
- The majority of detainees did not agree that synthetic cannabis is safer to use than natural cannabis, and 33 detainees reported experiencing some type of negative side effect
- Most common side effects included dizziness/nausea/vomiting (26%), paranoia/panic (18%) and headaches (15%). Other symptoms included delusional behaviour/anger outbursts, hallucinations and heart palpitations/chest pains requiring emergency care
- The range of negative side effects experienced by detainees from using synthetic cannabis products raises concerns for treatment providers and correctional officers who deal with drug-using offenders, given that consumers of synthetic cannabinoids could be placing themselves at risk of harm and displaying unpredictable behaviour
- Evidence from overseas suggests that banning a range of specific synthetic cannabinoid compounds has led to the increased availability of more harmful compounds with more severe side effects, on the market
Introduction
The recent emergence of products containing synthetic cannabinoids on the Australian and international markets has caused growing concern over the potential harms associated with its use. In addition, it raises a number of challenges for police with respect to policing the sale and consumption of such products which are often marketed as ‘legal highs’. While the possession and distribution of synthetic cananbinoids found to have similar pharmacological effects to cannabis is now illegal in Australia (TGA 2012), the complexities involved in preventing the sale of products containing new synthetic compounds still present a significant challenge for operational police. Some of the key concerns over the availability of synthetic cannabinoids for the health and criminal justice sectors are as follows:
- Products containing illegal synthetic cannabinoids are currently being sold in Australia via the Internet and marketed as legal to buy, claiming to contain ingredients not covered by state/territory bans
- Overseas research into synthetic cannabis products similar to those available on the Australian market revealed that some products contained ingredients not stated on the packaging (Dargan et al. 2011). This adds to the challenge for police in seizing products containing illegal synthetic cannabinoids
- Little is known about the short-term side effects resulting from consumption of synthetic cannabinoids currently being sold in Australia, and there is a dearth of information about the long-term side effects
- Drug-using prisoners may switch to synthetics to avoid drug detection in urine tests, thus increasing their risk of harm from products with unknown side effects, and potentially jeopardising their ability to be effectively rehabilitated in drug treatment programs
- In some jurisdictions adults who are found in possession of illegal synthetic cannabinoids are unable to be cautioned under cannabis cautioning schemes. This raises concerns over whether an increased number of young cannabis users who use synthetics will come into contact with the criminal justice system
While recent research has looked into the types of people who purchase and use synthetic cannabis products in Australia, little is known about the prevalence of synthetic cannabinoid use among the offender population, or what the perception of risks of using synthetic cannabis products are among drug-using offenders. In addition, only limited information is available on the potential negative side effects experienced as a result of consuming synthetic cannabinoids. In an attempt to fill the gaps in this area the Australian Institute of Criminology (AIC), in consultation with the National Cannabis Information and Prevention Centre (NCPIC), interviewed a sample of alleged offenders as part of the Drug Use Monitoring in Australia (DUMA) program, asking about their knowledge of, and experience using, synthetic cannabis products.
Background
Synthetic or ‘analogue’ drugs, as they are otherwise known, are a relatively new phenomenon to emerge on the global drug market. Products containing synthetic cannabinoids, designed to mimic the effects of cannabis, were first detected in Europe in 2008 being sold as ‘herbal incense’ or ‘room odorisers’ (EMCDDA 2012), although were likely available on the market as early as 2004 (Dillon & Copeland 2012). It is believed that similar products may have been available in Australia as early as 2004, although 2011 is when they began to attract attention from media and law enforcement (Dillon & Copeland 2012). Specifically, synthetic cannabinoids are psychoactive substances that mimic the effects of delta-9-tetrahydrocannabinol (THC), the active principle of cannabis, by binding to the same cannabinoid receptors in the brain and other organs as THC. Thus synthetic cannabinoids are functionally similar to THC when consumed (EMCDDA 2012).
The initial legal status of synthetic cannabis products, in combination with the absence of THC in the products, increased their appeal to individuals in Australia seeking to avoid detection in drug tests (such as mine workers) (AJM 2011) or consume drugs without breaking the law (Barratt et al. 2012). For a more detailed overview of the history of synthetic cannabinoids in Australia, see Dillon & Copeland (2012).
Following bans on synthetic cannabis products across Australian states/territories in 2011, police had the difficult task of detecting and seizing products containing illegal compounds of synthetic cannabinoids, only to find soon after that products containing new ingredients that were not covered by state/territory legislation began appearing on the shelves of various ‘head shops’ and on websites (Kirkwood 2011; Stark 2012). In 2012 the Theraputic Goods Association (TGA) implemented a federal ban on all synthetic cannabinoid products found to have similar pharmacological effects to THC when consumed (TGA 2012). It was intended that the new legislation, which came into effect in May 2012, would deter manufacturers from synthesising and selling new compounds not covered under state/territory bans.
Being relatively new to the drug market, little is known about the side effects of using synthetic cannabinoids. A survey of synthetic cannabis users in Australia found that 68 per cent of the sample experienced at least one side effect after use, which included decreased motor-coordination, increased heartbeat, dissociation, dizziness, paranoia and psychosis (Barratt et al. 2012). Another study analysed case reports from patients presenting to Nepean Hospital in Sydney, with results indicating that while use of natural cannabis was linked with psychosis, use of synthetic cannabinoids was linked with psychosis with an increased level of agitation (Brakoulias 2012).
Overseas research suggests a shift in the market towards more potent synthetic cannabinoid compounds that produce more harmful side effects (Hermanns-Clausen et al. 2012). Similar suggestions have been made in Australia as manufacturers attempt to circumvent state/territory legislation by releasing new, untested products that are potentially more harmful (Stark 2012).
Method
Data for this Bulletin were collected as part of the Australian Institute of Criminology’s (AIC) DUMA program, a self-report survey of drug use and criminal offending among police detainees who had been charged by police (but not yet convicted). DUMA has operated continuously for over 13 years and data collection occurs at nine sites across Australia (Sweeney and Payne 2011). The results are used to inform the development of strategic responses to new and emerging drug/crime issues. Further information about DUMA and its methodology can be found elsewhere (Makkai 1999).
Specifically, data used in this Bulletin are derived from police detainees interviewed at eight data collection sites between January and February 2012 – Southport and Brisbane (Queensland), Bankstown and Kings Cross (New South Wales), East Perth (Western Australia), Footscray (Victoria), Adelaide (South Australia) and Darwin (Northern Territory). The AIC, in consultation with NCPIC, designed an addendum questionnaire to the core DUMA survey, which asked detainees specifically about their use of cannabis, and in particular, synthetic cannabis.
Results
A total of 871 police detainees participated in the addendum questionnaire. Aggregated across all sites, almost half (49%) had heard of synthetic cannabis, while only four per cent (N=36) reported using synthetic cannabis in the last 30 days. In contrast, almost half of the sample (46%; N=407) reported recent use of bush weed or hydroponic cannabis (see Table 1). Detainees were not asked if they had used synthetic cannabis beyond the 30-day period, although this would likely have produced a larger proportion.
Only 12 detainees indicated the name of the product they used, the most common being Kronic (7 detainees). Other product names included Diablo, Godfather, K2, Ash and Zero Gravity. All detainees reported smoking as the method of consumption (see Table 3).
Table 1: Prevalence of cannabis and synthetic cannabis use

Table 2: Name of synthetic cannabis consumed
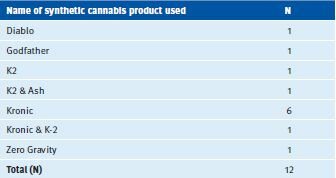
Table 3: Method of consumption of synthetic cannabis
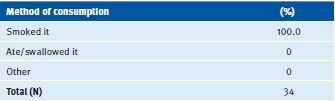
Table 4: Sources for synthetic cannabis consumed in the last 30 days
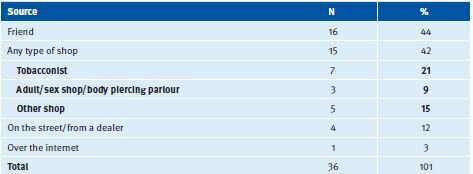
Of the 36 detainees who reported recent use of synthetic cannabis, the largest proportion reported obtaining it through a friend (44%) or from some type of shop (42%), including tobacconists (21%), adult sex shops or body piercing parlours (9%), or another type of shop (15%). Findings indicate that products were still being sold in shops despite the introduction of state/territory legislation to ban the sale and possession of synthetic cannabinoids. Twelve per cent of detainees obtained synthetic cannabis from a dealer, and only one detainee purchased synthetic cannabis via the internet (see Table 4).
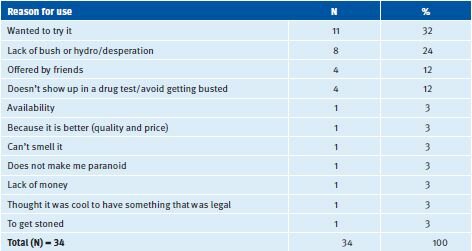
Similarly a recent study in Australia (Barratt et al. 2012) found that synthetic cannabis was most commonly purchased from ‘head shops’ or drug paraphernalia stores, although unlike DUMA detainees, 22 per cent of the sample in that study had obtained the products via the internet (Barratt et al. 2012). This most likely reflects the nature of the detainee sample compared to those in the Barratt et al. (2012) study, who were recruited via an online survey. The most commonly reported reason for using synthetic cannabis among DUMA detainees was simply wanting ‘to try it’ (32%), or that there was a lack of ‘bush weed’ or ‘hydro’ available (24%). Other reasons included being offered it by friends (12%) and the fact that it did not show up in a drug test (12%) (see Table 5).
Table 5: Main reasons for using synthetic cannabis instead of cannabis
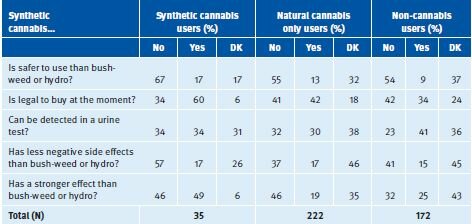
The AIC was interested in what the perception was among offenders regarding the effects, risks and legality of synthetic cannabis. All detainees who had heard of synthetic cannabis (N=429), including non-users, where given several scenarios and asked to answer ‘yes’ or ‘no’ to these. Detainees were separated into three groups: ‘synthetic cannabis users’ (some of whom had used cannabis as well); natural cannabis-only users; and ‘non-cannabis users’ (those who did not use synthetic cannabis or cannabis). The first statement was, “Synthetic cannabis is safer to use than bush weed or hydro”. The majority of detainees did not agree with this statement, with synthetic cannabis users being the most likely (67%) to answer ‘no’ to the statement, followed by natural cannabis-only users (55%). Results indicated that even among non-cannabis users in the sample (N=172), the majority (54%) had perceptions that synthetic cannabis is not safer to use than natural cannabis. Only nine per cent of non-cannabis users agreed that synthetic cannabis is safer to use and 37 per cent were unsure (see Table 6).
In support of this finding, only 15-17 per cent of detainees in all three groups agreed that synthetic cannabis has less negative side effects than bush weed or hydro, compared to the majority (57%) of synthetic cannabis users disagreeing with the statement, and 37 per cent of natural cannabis-only users and 41 per cent of non-cannabis users disagreeing. Almost half (46% and 45% respectively) of natural cannabis-only users and non-cannabis users were unsure whether synthetic cannabis has less negative side effects. Perceptions of whether synthetic cannabis has a stronger effect than natural cannabis were inconsistent across the groups, with similar proportions of synthetic cannabis users disagreeing (49%) and agreeing (46%) that synthetic cannabis has a stronger effect. This compares to natural cannabis-only users, of whom 46 per cent disagreed and 19 per cent agreed, and non-cannabis users, of whom 32 per cent disagreed and one quarter (25%) agreed that synthetic cannabis has a stronger effect. There appeared to be a lack of consensus over whether synthetic cannabis has stronger effects.
Interestingly, synthetic cannabis users were the most likely (60%) to believe that synthetic cannabis was legal to buy at the time of interview, compared to 42 per cent of natural cannabis only users and just over one third (34%) of non-cannabis users. Findings indicate a degree of confusion over the perceived legality over the drug, which had been made illegal in all jurisdictions prior to interviewing.
Finally, just over one third (34%) of synthetic cannabis users believed synthetic cannabis could not be detected in a urine test, and over one third (34%) believed it could be detected, with another 31 per cent unsure (see Table 6).
Table 6: Perceptions regarding synthetic cannabis
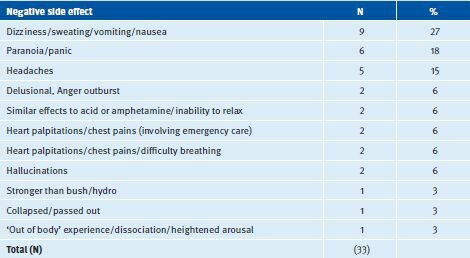
Detainees were asked whether they had personally experienced any negative side effects from using synthetic cannabis. Thirty-three detainees reported experiencing negative side effects in the form of a range of different symptoms, with the most common being dizziness/sweating/ vomiting/nausea (27%), followed by paranoia/panic (18%) and headaches (15%). Two detainees reported being delusional or having an anger outburst, another two experienced effects similar to taking ‘acid’ or amphetamines with an inability to relax and another two experienced hallucinations. Another four detainees reported experiencing heart palpitations, chests pains and difficulty breathing, with two of these cases requiring emergency care. Other negative side effects included experiencing stronger effects than ‘bush weed’ or ‘hydro’, collapsing/‘passing out’ and ‘out of body’ experience (see Table 7).
Table 7: Negative side effects experienced from using synthetic cannabis
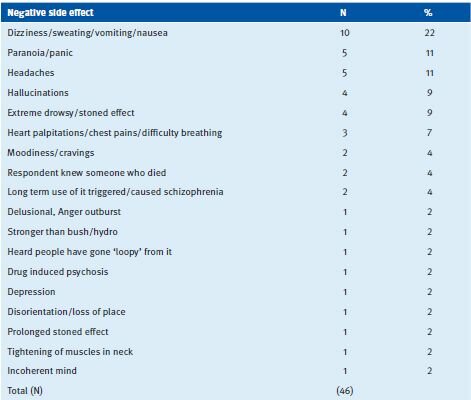
All detainees who had heard of synthetic cannabis (including non-users) were asked if they knew anyone else who had experienced negative side effects from using synthetic cannabis, to which 5 per cent (N=46) of detainees said yes. The most common side effect experienced by someone the detainees knew was dizziness/sweating/vomiting/nausea (22%), followed by paranoia/panic (11%) and headaches (11%). While the side effects experienced by someone the detainees knew were generally similar to those reported by detainees who had used synthetic cannabis themselves, there were some additional symptoms reported. For example, two detainees reported that use of synthetic cannabis triggered schizophrenia in someone they knew. Other reported side effects included drug-induced psychosis, depression and ‘going loopy’. Two detainees reported knowing someone who had died from using synthetic cannabis (see Table 8). It should be noted that the data are based on self-reports from detainees, and cannot necessarily be verified; although the media has reported at least one death from synthetic cannabis use in Australia (Trenwith 2011).
Table 8: Negative side effects experienced by someone else detainees knew
Conclusion
In response to the growing concern over the availability and use of products containing synthetic cannabinoids in Australia, the Australian Institute of Criminology, in consultation with NCPIC, surveyed a sample of offenders through the DUMA program to ask about their experience with using synthetic cannabis. Of the 871 detainees, four per cent reported recent use of synthetic cannabis. This compares to almost half of the sample (46%) reporting recent use of cannabis (‘bush weed’ or ‘hydro’). Coupled with the disagreement among the majority of detainees that synthetic cannabis is ‘safer’ to use than cannabis, the finding highlights a lack of trust towards products containing synthetic cannabinoids, even among non-cannabis users in the sample, but particularly among those who had used synthetic cannabis. It also supports findings from a study of drug users surveyed through the Global Drug Survey, which found that 93 per cent of users would choose cannabis over synthetic cannabis (GDS 2012).
The finding may also suggest that synthetic drugs are more popular among different segments of the population who do not come into frequent contact with the criminal justice system. Barratt et al (2012), for example, found that among a sample of 316 synthetic cannabis users, the majority were employed and had high educational attainment. This is in contrast to offenders in the DUMA sample, typically characterised by high levels of unemployment and low levels of educational attainment. In addition, that only one detainee obtained synthetic cannabis via the internet (with the most common source being a friend (44%) or some type of shop (e.g. tobacconist, sex shop) (42%) indicates that internet sites selling synthetic drugs appeal to, and are marketed towards, a different demographic than offenders in the DUMA sample.
This lack of trust towards consumption of synthetic cannabis products among offenders in the DUMA sample is likely derived from the concerning negative side effects reported by detainees after use (ranging from dizziness/nausea/vomiting and chest pains/heart palpitations to paranoia/panic and delusional outbursts). These findings have implications for health practitioners, law enforcement officers and correctional staff who deal with drug-using offenders, with the potential for individuals who consume synthetic cannabinoids to display unpredictable behaviour. Of those who did use synthetic cannabis, the majority still believed the drug was legal to buy at the time of interview, pointing to a need for more awareness-raising over the illegality of the drug.
It is difficult to determine what the most effective policy solution is for Australia in preventing the sale of, and harm associated with, the use of synthetic cannabis and other analogues. While the TGA has now included all synthetic cannabinoid products with a similar pharmacological effect to cannabis to Schedule 9 of the Standard for Uniform Scheduling of Medicines and Poisons (TGA 2012), it will take time for states and territories to implement this legislation. As stated by the Alcohol and Other Drug Council of Australia (ADCA) (2011), there is a need for further investigation into evidence-based methods for the effective reduction in harm associated with the sale and consumption of synthetic cannabinoids.
In the meantime however, products continue to be sold online and in tobacconists, often marketed as ‘legal highs’ and ‘containing only herbal ingredients’ (Stark 2012), thus contributing to the misperceptions that synthetic cannabinoids are, a) similar to cannabis; b) safe to use; and c) legal to buy. As Seely et al. (2012) suggest, raising awareness among physicians, those in the justice sector and the general Australian community as to the illegality of synthetic cannabinoids, as well as the negative side effects from using these products, will hopefully assist in reducing the prevalence of use and harm associated with the use of synthetic cannabinoid products.
References
- Alcohol and other Drugs Council of Australia ADCA. (2012). Submission No. 18 Enquiry into law reform issues surrounding synthetic drugs by the NSW Legislative Assembly Legal Affairs Committee. 20 April 2012. Canberra: ADCA. Available at: http://www.adca.org.au/index.php?option=content&task=view&id=332
- Australian Journal of Mining AJA. (2011). WA Government bans Kronic. Available at:http://www.theajmonline.com. au/mining_news/news/2011/june/june-16-2011/top-stories/wa-government-bans-kronic
- Barratt, M., Cakic, V. & Lenton, S. (2012). Patterns of synthetic cannabinoid use in Australia. Drug and Alcohol Review 10, 1465-3362.
- Brakoulias, V. (2012). Products containing synthetic cannabinoids and psychosis. Australian and New Zealand Journal of Psychiatry 46, 281-282.
- Dargan, P., Hudson, S., Ramsey, J., & Wood, D. (2011). The impact of changes in UK classification of the synthetic cannabinoid receptor agonists in ‘Spice’. International Journal of Drug Policy 22, 274-277.
- Dillon, P. & Copeland, J. (2012). Synthetic cannabinoids: The Australian experience. Bulletin Series 13. Sydney: National Cannabis Prevention and Information Centre.
- Europoean Monitoring Centre for Drugs and Drug Abuse EMCDDA. (2012). Synthetic cannabinoids and Spice. EMCDDA. Accessed 9 December 2012. Available at:http://www.emcdda.europa.eu/publications/drug-profiles/synthetic-cannabinoids
- Global Drug Survey GDS. (2012). 2012 Global Drug Survey. London: GDS. Available at:http://globaldrugsurvey.com/run-my-survey/2012-global-drug-survey
- Hermanns-Clausen, M., Kneisel, S., Szabo, B., & Auwarter, V. (2012). Acute toxicity due to the confirmed consumption of synthetic cannabinoids: Clinical and laboratory findings. Addiction 10, 534-544.
- Kirkwood, I. (2011). Ban on synthetic cannabis Kronic fails. Newcastle Herald. December 18 2011. Available at: http://www.theherald.com.au/story/441994/ban-on-synthetic-cannabis-kronic-fails/
- Makkai, T. (1999). Drug Use Monitoring Australia: A brief description. Research and Public Policy Series No. 21. Canberra: Australian Institute of Criminology. Available at:http://www.aic.gov.au/publications/current%20series/rpp/21-40/rpp21.aspx
- Stark, J. (2012). Ban on fake pot fails to drag off shelf. The Age. April 1 2012. Available at:http://www.theage.com.au/victoria/ban-on-fake-pot-fails-to-drag-drug-off-shelf-20120331-1w5ct.html
- Sweeney, J. & Payne, J. (2012). Drug use monitoring in Australia: 2009 and 2010 annual report on drug use among police detainees. Monitoring report. Canberra: Australian Institute of Criminology.
- Theraputic Goods Association TGA. (2012). Reasons for scheduling delegates’ final decisions. February 2012. Canberra: Department of Health and Ageing. Available at:http://www.tga.gov.au/industry/scheduling-decisions-1202-final.htm
- Trenwith, C. (2011). More substances banned following first Kronic death. WA Today. Available at:http://www.watoday.com.au/wa-news/more-substances-banned-following-first-kronic-death-20110805-1ie5m.html.